BIMONTHLY ASSESMENT JANUARY 2021
1)26 year old woman with complaints of altered sensorium somce 1 day,headache since 8 days,fever and vomitings since 4 days
a). What is the problem representation of this patient and what is the anatomical localization for her current problem based on the clinical findings?
Ans:
problem presentation
in order of priority at the time of admission:
1)altered sensorium with irrelevant talk since 1 day
2)neck pain with headache since one month which worsened for the past 8 to 15
3)vomitings since one week
4)low grade fever since one week
5)generalised weakness with decreased appetite since one month
anatomical localisation of current problems
Brain-meninges and ?frontal lobe, due to altered sensorium
B)What is the etiology of the current problem and how would you as a member of the treating team arrive at a diagnosis? Please chart out the sequence of events timeline between the manifestations of each of her problems and current outcomes.

Picture about etiology from Bradley's textbook of neurology
going by the table mentioned
the cause for altered sensorium can be attributed to hyponatremia,therefore sodium correction would be done ,
but persistent delirium after correction would probe to considering other causes as well
and particularly around cause for hyponatremia.
the history of neck pain ,headache, vomiting,fever would point towards checking for meningeal involvement
clinical examination - signs
intervention-lumbar puncture
imaging-mri with contrast
Various mechanism have been postulated as how TB can induce hyponatremia, like local invasion to the adrenal glands, local invasion to hypothalamus or pituitary gland, [8][9][10][11] meningitis [12][13][14] and inappropriate ADH secretion due to pulmonary infection [15][16][17], TB can affect adrenal glands directly. TB may destroy adrenals and leading to overt or subclinical adrenal insufficiency and it is one of the most common cause of Addison’s disease in India [2]. The present study was done to study and analyze the prevalence of hyponatremia in adult patients with PTB in tertiary care in India.
one of the cause for siadh could be extrapulmonary tb.
C)What is the efficacy of each of the drugs listed in her prior treatment plan that she was following since last two years before she stopped it two weeks back?
hcq
Of the 509 patients who met inclusion criteria, 66.2% (n = 337) continued HCQ throughout the duration of their treatment (median duration of HCQ treatment was 8.0 years), whereas 33.8% (n = 172) did not (median duration of HCQ treatment was 1.9 years). Patients who received HCQ for less than 1 year before discontinuation (median duration of HCQ treatment was 2.5 months) were more likely to experience SLE flares compared with those who continued HCQ for more than 1 year (13.1% vs 5.7%, P = 0.019). Patients who experienced a flare while on HCQ were more likely to have arthritis, oral ulcers, leukopenia, and thrombocytopenia.
Methylprednisolone
173 patients, 92 CC and 81 BC, were studied. The clinical presentation of both cohorts was similar, with no significant differences in the mean SLEDAI score at diagnosis (6.6 vs. 8.1, p = 0.06). Patients from CC were treated more frequently with hydroxychloroquine (mean 57 vs. 43 months), methotrexate (24% vs. 11%) and pulse methyl-prednisolone (42% vs. 26%), and received lower doses of oral prednisone (average dose during the follow up 2.3 vs. 7.2 mg/d, p < 0.001). Patients in CC were more likely to achieve ClinROnT at year one, 84% vs. 43% (p < 0.001). Prolonged ClinROnT during the 5 years of follow up was more frequent in CC: 70% vs. 28%, p < 0.001. Patients in CC were also more likely to achieve ClinROnT after controlling for baseline SLEDAI (adjusted HR 1.69, 95%CI 1.21-2.35) and for the presenting clinical manifestations (adjusted HR 1.72, 95% CI 1.2-2.4).
alendronate for increasing bone density in gluco corticoid induced osteoporosis
We carried out two 48-week, randomized, placebo-controlled studies of two doses of alendronate in 477 men and women, 17 to 83 years of age, who were receiving glucocorticoid therapy. The primary end point was the difference in the mean percent change in lumbar-spine bone density from base line to week 48 between the groups. Secondary outcomes included changes in bone density of the hip, biochemical markers of bone turnover, and the incidence of new vertebral fractures.
Results: The mean (+/-SE) bone density of the lumbar spine increased by 2.1+/-0.3 percent and 2.9+/-0.3 percent, respectively, in the groups that received 5 and 10 mg of alendronate per day (P<0.001) and decreased by 0.4+/-0.3 percent in the placebo group. The femoral-neck bone density increased by 1.2+/-0.4 percent and 1.0+/-0.4 percent in the respective alendronate groups (P<0.01) and decreased by 1.2+/-0.4 percent in the placebo group (P<0.01). The bone density of the trochanter and total body also increased significantly in the patients treated with alendronate. There were proportionally fewer new vertebral fractures in the alendronate groups (overall incidence, 2.3 percent) than in the placebo group (3.7 percent) (relative risk, 0.6; 95 percent confidence interval, 0.1 to 4.4). Markers of bone turnover decreased significantly in the alendronate groups (P<0.001). There were no differences in serious adverse effects among the three groups, but there was a small increase in nonserious upper gastrointestinal effects in the group receiving 10 mg of alendronate.
Conclusions: Alendronate increases bone density in patients receiving glucocorticoid therapy.
Cholecalciferol
To determine the efficacy and safety of vitamin D 50,000 units/week and calcium 1,000 mg/day in the prevention of corticosteroid induced osteoporosis.
Methods: A minimized double blind, placebo controlled trial in corticosteroid treated subjects in a tertiary care university affiliated hospital. The sample was 62 subjects with polymyalgia rheumatica, temporal arteritis, asthma, vasculitis, or systemic lupus erythematosus. The primary outcome measure was the percentage change in bone mineral density (BMD) of the lumbar spine in the 2 treatment groups from baseline to 36 mo followup.
Results: BMD of the lumbar spine in the vitamin D and calcium treated group decreased by a mean (SD) of 2.6% (4.1%) at 12 mo, 3.7% (4.5%) at 24 mo, and 2.2% (5.8%) at 36 mo. In the placebo group there was a decrease of 4.1% (4.1%) at 12 mo, 3.8% (5.6%) at 24 mo, and 1.5% (8.8%) at 36 mo. The observed differences between groups were not statistically significant. The difference at 36 mo was-0.693% (95% CI -5.34, 3.95).
fluperitine and diclofenac for pain
A controlled, parallel group study of the analgesic efficacy of flupirtine maleate, was compared against diclofenac sodium in 40 orthopaedic patients with post-operative pain. Clinically, both drugs were of equal analgesic efficacy
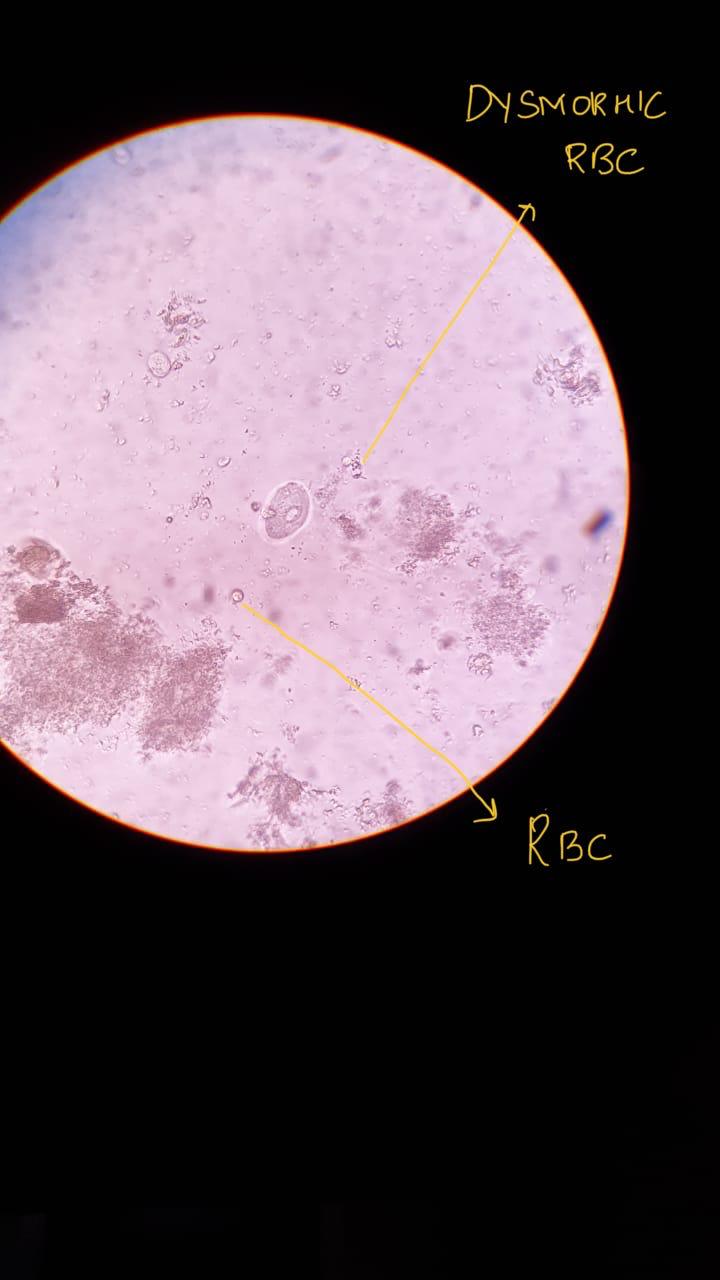
D)Please share any reports around similar patients with SLE and TB meningitis?
The following is a case report of tb meningitis in a 15yr old girl who is a known case of sle since 4 years
Any reports of normal csf leukocyte count and normal csf protein in meningitis?
The following table reports, ADA to be more specific in diagnosis of TB meningitis from csf sample, with value greater than 6
Our patient's value of ADA being 9 , rules in favour of tb meningitis
What could be the probable cause for a normal csf leukocyte count in a patient with chronic meningitis?
e)What is the sensitivity and specificity of ANA in the diagnosis of SLE?
Of 1010 ANA test results reviewed, 153 were positive. The group with positive ANA test results included more patients aged 65 years or older than the group with negative ANA test results (30% vs 15%, P < .003). The diagnosis of systemic lupus erythematosus (SLE) was established in 17 patients, all of whom had positive ANA test results. Other rheumatic diseases were found in an additional 22 patients. The estimated sensitivity and specificity of the ANA test for SLE were 100% and 86%, respectively. For other rheumatic diseases, sensitivity and specificity were 42% and 85%, respectively. The positive predictive value of the ANA test was 11% for SLE and 11% for other rheumatic diseases. Specificity and positive predictive value for ANA testing in the elderly patients were lower than among younger patients.
What was the research question in the above thesis presentation?
The research question
1)will salt restricted diet decrease blood pressure?
2)can 24hr urinary sodium test reflect the amount of sodium consumed by an individual
What was the researcher's hypothesis?
Hypothesis is that, salt restriction doesn't effect blood pressure in all the individuals in the same way, and salt resistant individuals don't benefit from a restricted diet as much as a salt sensitive individual.
What is the current available evidence for the utility of monitoring salt excretion in the hypertensive population
The 24hr urinary sodium is a reflection of dietary sodium, and has better results than dietary recall method
Daily salt intake based on 24-hour urinary sodium excretion (assuming that all sodium ingested was in the form of sodium chloride) with a formula: figure 2 shows a practical method to estimate salt or sodium intake.
Figure 2: Calculation for estimation of salt or sodium intake
Na (mg/day) = Na (mmol/day) x 23; NaCl = Na (g/day) x 100/ 39,3
1 gram salt (NaCl) = 393,4 mg Na = 17,1 mmol Na
What was the research question in the above thesis presentation?
The research question in the above thesis is whether magnesium plays a role in complications of diabetes mellitus
What was the researcher's hypothesis?
The researcher's hypothesis is that hypomagnesemia causes complications of dm2 irrespective of other confounding factors like age,duration of diabetes.
What is the current available evidence for magnesium deficiency leading to poorer outcomes in patients with diabetes?
In this retrospective study 673 diabetic patients were evaluated.
According to Mg levels, the patients were divided into two groups; as normomagnesemic patients and hypomagnesemic patients.
There were 55 patients (8.2%) with diabetic retinopathy and 95 patients (14.1%) with diabetic neuropathy. Five hundred patients (74.3%) had normoalbuminuria; 133 patients (19. 8%) had microalbuminuria (MA) and 40 patients (5.9%) had overt proteinuria. One hundred and seventy one patients (25.4%) had HbA1c levels equal or below 7%; and 502 patients (74.6%) had HbA1c levels above 7%. There was no statistical difference in age or duration of diabetes between the groups formed according to Mg levels. Although there were no differences between the groups for retinopathy and neuropathy, MA was more common in hypomagnesemic patients (p =0.004). HbA1c levels did not differ between the groups (p =0.243). However there was a weak negative correlation between serum Mg and HbA1c levels (r =-0.110, p =0.004) and also between serum Mg and urine protein level (r =-0.127, p =0.018
3)Please critically appraise the full text article linked below:
What is the efficacy of aspirin in stroke in your assessment of the evidence provided in the article. Please go through the RCT CASP checklist here https://casp-uk.net/casp-
Clinical appraisal of the article:
1)The study answered the research question
being the use of asprin for prevention of stroke progression.
it was foccused in terms of intervention given and outcome measured
2)the method for randomisation was appropriate eliminating systematic bias and allocation sequence concealed from investigators and participants
3)all the participants included in the study were accounted for, including rhe two parcels whixh were accidentally opened.
4)the participants and the investigators were blind methodically
5)the study groups were similar
6)apart from the experimentation, the hospital care given is not documented
7)there were dropouts in the study, study medication was interrupted in few due to suspected side effects,
the p value was not mentioned
8)the cI interval 95%0.6-1.45
9)the treatment effect wasn't much,
10)the outcomes are benefial to my population in prescribing anticoagulants
dual vs single antiplatelet use and longer duration of followup could have been made .
4) Please mention your individual learning experiences from this month.
January 1st 2021:
was posted in Unit 3 from this month Attended rounds
cause of hyponatremia in SLE patient
Learnt about SLICC criteria
Attended 2-4 pm session
January 2nd:
Discussed regarding SLE patient with TB meningitis in 2-4 pm session.
Discussed about the SIADH secondary to SLE
January 3rd:
Attended rounds
Reviewed literature on post dialysis leading to improvement in kidney function or renal shut down.
January 4th:
Attended rounds
And reviewed literature on hyponatremia
January 5th:
Discussed about an elderly woman with AKI on CKD
Attended rounds
Reviewed literature on a post op case( referral)
Hypotension refractory to fluids
January 6th:
Was my Opd duty day
Saw Opd cases
Evaluated a case of a 18 yr old boy
For paraparesis
Review literature
Admitted 2 cases
January 7th:
Attended rounds
Evaluated both the cases
First case : 65 year old man with CKD secondary to diabetes and NSAID use
Known case of type 2 DM and hypertension
? Anemia of Chronic disease
Review of literature
Second case: 15 year old boy with Paraparesis since 6 months and a history of fever 6 months back
Discussed about the Paraparesis case with the Neurologist and came with a provisional of -
1. Compressive Myelopathy
2.? Non compressive Myelopathy -? Post infectious myelitis
3. Subacute combined degeneration
Discussed regarding 15 year old boy with Paraparesis in 2-4pm session and on rounds.
January 8th:
Examined 15 year old boy with Paraparesis
Link to the elog 👇
https://priyankadevarapalli.blogspot.com/2021/01/15-yr-male-with-paraplegia.html
Got MRI spine done for the patient in order to look for any compressive lesions causing myelopathy
January 9th:
Attended rounds
Discussed about various causes of paraparesis
Learnt that ACA infarct especially in cases with a single ACA
could present like this along with posterior spinal artery infarct which in which the patients would have dorsal column as in our case
January 10th
Attended rounds
January 11th:
Attended rounds
Attended 2-4pm class
January 12th
Attended rounds
Discussed about a CLD case who is HCV positive and am alcoholic in 2-4pm session
Discussed on Anti HCV drugs
January 13:
It was my duty day
Admitted a 55 year man with? Acute glomerulonephritis
A 55 year old male working as an LIC assistant presented to casualty
C/o altered taste sensation since 7 days
c/o abdomen distension since Wednesday morning
B/L Pedal oedema
Pitting type since 2-3 days
SOB grade 3 since 2-3 days
H/o change in voice since morning
Denies history of hematuria, frothy urine
H/o RTA 2 days back sustained injuries to right leg
K/c/o T2DM since one year and on regular medication
O/e
BP 140/70 mmhg
PR - 124bpm
RR - 28 cycles per min
CVS - S1S2 +
RS - BAE






+
January 14:
Discharged the patient on discharge at request
Attended rounds
Discussed with the nephrologist on about pathogenesis of NSAIDs leading to CKD
Most nephrotoxic aminoglycoside is Gentamycin
January 15:
Attended rounds
Discussed how to differentiate Right heart failure from left heart failure on cvs examination
Discussed about a below knee amputation case with Recurrent Atrial Fibrillation
January 16th
Attended rounds
Discussed about 15 year boy with Paraparesis in the class and the use of csf analysis in him
Reviewed literature on sepsis acting as a trigerring factor for Atrial fibrillation
5) a) What are the possible reasons for the 36 year old man's hypertension and CAD described in the link below since three years?
The possible reasons for hypertension and cad in the given history could be
Alcohol
The HPFS is a prospective investigation of 51 529 US male dentists, pharmacists, veterinarians, optometrists, osteopathic physicians, and podiatrists aged 40 to 75 years who returned a mailed questionnaire about diet and medical history in 1986.
At baseline, men reported their alcohol consumption on a 131-item semiquantitative food frequency questionnaire (FFQ) that included separate items for beer, white wine, red wine, and liquor. Participants were asked how often, on average over the past year, they consumed each beverage. We calculated total alcohol intake by multiplying the average consumption of each beverage by the alcohol content of the specified portion size (12.8 g for beer, 11.0 g for wine, and 14.0 g for liquor) and summing across beverages. The FFQ was administered again every 4 years, with an item for light beer added in 1994. Participants also reported their overall drinking frequency in 1986, 1988, and 1998.
results:
When we compared alcohol intake of 5.0 g/d or more vs less than 5.0 g/d, the hazard ratio was 0.58 (95% CI, 0.37-0.89). Given that 55% of person-time was contributed by consumers of 5 g/d or more of alcohol, we estimate that 25% of the incidence cases of MI in this population were attributable to consuming less than 5 g/d (95% CI, 11%-47%).
Smoking
Temporal Associations Between Smoking and Cardiovascular Disease, 1971 to 2006 (from the Framingham Heart Study)
b) Please describe the ECG changes and correlate them with the patient's current diagnosis.
The ecg suggests:
1st ecg-irregularly irregular rythmn,normal axis,
Intermittent broad qrs complexes ? ventricular escape rythmn,?idioventricular rythmn
Remaining ecg-poor r wave progression with regular rythmn
c) Share an RCT that provides evidence for the efficacy of primary PTCA in acute myocardial infarction over medical management. Describe the efficacy in a PICO format.
RITA-2 is a randomized control trial published in
Journal of the American College of Cardiology Clinical Trials Vol. 42, No. 7, 2003 © 2003 by the American College of Cardiology Foundation Published by Elsevier Inc.
P-1018,Patients were recruited at 20 centers in the U.K. and Ireland. In brief, patients with arteriographically proven coronary artery disease (CAD) were considered for the trial if the supervising cardiologist thought that continued medical therapy and PTCA were both acceptable treatment options. Patients had to be over 18 years of age, but there was no upper age limit.
I-The 1,018 patients were randomized to coronary angioplasty (n 504) or continued medical treatment (n 514) from July 1992 to May 1996. Follow-up to September 30, 2001, is included in this report, the median follow-up period being seven years.
C-compared based on death and MI
subsequent interventions required
relief of symptoms of angina and breathlessness
O-Death or myocardial infarction (MI) occurred in 73 (14.5%) PTCA patients and 63 (12.3%) medical patients (difference 2.2%, 95% confidence interval 2.0% to 6.4%, p 0.21). There were 43 deaths in both groups, of which 41% were cardiac-related. Among patients assigned PTCA 12.7% subsequently had coronary artery bypass grafts, and 14.5% required additional non-randomized PTCA. Most of these re-interventions occurred within a year of randomization, and after two years the re-intervention rate was 2.3% per annum. In the medical group, 35.4% required myocardial revascularization: 15.0% in the first year and an annual rate of 3.6% after two years. An initial policy of PTCA was associated with improved anginal symptoms and exercise times. These treatment differences narrowed over time, mainly because of coronary interventions in medical patients with severe symptoms.

Comments
Post a Comment